Please scroll on the PDF below to view the entire document!
Social Prescribers
How we can help.
- Help and support with non-medical issues e.g. housing, debts, mental health, bereavement, refugee/asylum seeker issues and benefits.
- Support clients to access Health & Social Care where needed. This will include supporting patients at meetings and acting as advocates.
- Offer peer support groups e.g. sleep well and mental health
- Work with other third sector organisations in the community to break down barriers for patients and help them to access information they need.
How we can help.
- To assess patients with soft tissue, muscle and joint pain and to decide on the most appropriate management pathway.
- FCPs are physiotherapists with expertise in the assessment and management of Musculoskeletal (MSK) conditions.
Routine steroid injections can be administered to certain joints e.g. knee, shoulder. However, there are some joints which CANNOT be administered; hip, elbow, small hand joints and spinal.
There are also contraindications to injection therapy e.g. unstable diabetic patients.
If you send patients with regards to an injection, explain to the patient that it is an assessment with regards to whether this is the most appropriate treatment for them.
Please see attached document for further guidance:
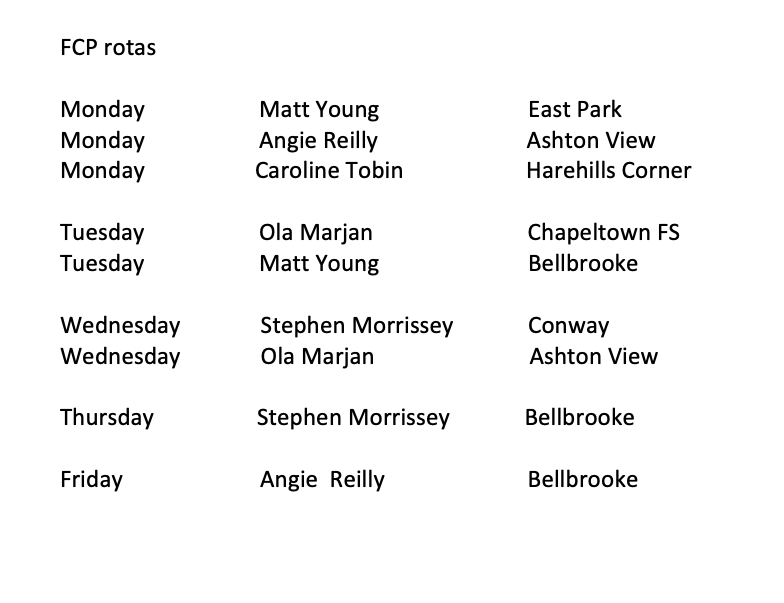
FCP Rotas
Leeds Mental Wellbeing Service (LMWS)
How we can help.
- We address the mental health needs of patients with complex histories, co-morbidity, patients who haven’t previously met criteria for or have disengaged with IAPT or CMHTs.
- Support patients who find it difficult navigating into mental health services by themselves.

Trauma Informed Approach
Trauma Charter
As a PCN, we are committed to implementing trauma informed care and agree to the commitment described in the charter.
Healthy Minds
Healthy Minds appointments are available Monday – Friday during core hours. These appointments support patients who are struggling with low level mental health and emotional wellbeing difficulties.
DO NOT BOOK under 18s, patients who are expressing thoughts of self-harm, or patients who are under the secondary care mental health team. Any questions reach out to teresa.dcaccia@nhs.net.
PLEASE ALWAYS DOUBLE UP THE APPOINTMENT FOR PATIENTS NEEDING LANGUAGE LINE OR INTERPRETATION FROM A FAMILY MEMBER
HEROES
HEROES Level 1
How we can help:
- The HEROES Peer Support Programme is a series of courses, workshops and generalised support groups for patients struggling with their mental health.
- HEROES stands for Healing, Education and Recovery Of Emotional Strength and it also stands for the kind of person who joins our groups!
- Groups are run by trained facilitators in a safe, compassionate and recovery-focused space.
We explore topics such as Self-Compassionate practice, Mindfulness, Anxiety Management, Confidence Building and Assertiveness Skills. New courses will be added throughout the year.
Please contact the Care Coordination hub – for further details.
We look forward to welcoming more patients who may be suffering emotionally. All mental health diagnoses welcome!
HEROES Level 2
HEROES Level 2 is now being piloted and co-produced with patients from the BHR PCN. Following the success and outcomes of the 8 week HEROES Groupwork Programme, founder Miranda Arieh is now piloting this follow up.
Within this level we will explore further applying the motivational coaching approach to mental health recovery, while exploring topics such as trauma release, managing anger, nervous system regulation, meditation, how to create a positive mindset, dealing with triggers, managing emotional flashbacks and much more.
You need to have graduated from level one of the HEROES Programme prior to entering level 2.
Find out more at here or ask your GP for further info.
SMI
BHR PCN have a small team to support patients that have a diagnosis of a serious mental illness (SMI): Schizophrenia, bipolar disorder and other psychoses. Around 400,00 people in England are living with Schizophrenia and around 544,631 people are living with bipolar disorder. People living with a SMI are at considerably increased risk of physical ill health than the general population and have demonstrably poorer health and health outcomes. Our team of healthcare assistants, nursing associates and care coordinators are a dedicate team that are here to help our patients to access primary care services and reduce health inequalities for this population.
The team focus is supporting patients to have annual health reviews which include a physical health check: Bloods test, Blood Pressure, check patients are accessing cancer screening appointments. It also includes a review of their mental health care plans and includes development of personalised care plans. The team do this by assisting patients to seek help with lifestyles changes, emotional support and can support patients in accessing health and wellbeing coaching.
Importance of having a annual health check:
Why is it important for you to attend for your SMI health review
We Offer
- GP appointments:
Monday, Tuesday, Wednesday, Thursday and Friday
Saturday and Sunday - ANP (Advanced Nurse Practitioner) Tuesday and Thursday
- LARC, (Long acting reversible contraception) coil & implants insertion/removal:
Saturday and Sunday - Practice Nurse:
Saturday and Sunday - HCA:
Saturday and Sunday
How we can help.
- Support practices with medication related process such as medication queries, medication reviews and repeat prescription reauthorisations. Supporting practices with processing clinical documents and structured medication reviews.
- Safety audits including MHRA and amber drug monitoring.
- Project work highlighted by national quality and safety directives.
- Supporting with all aspects of prescribing for the care homes team.
Pharmacy First
The Pharmacy First service builds on the NHS Community Pharmacist Consultation Service which has run since October 2019. The consultation service enables patients to be referred into community pharmacy for a minor illness or an urgent medicine supply.
The new Pharmacy First service, launched 31 January 2024, adds to the existing consultation service and enables community pharmacies to complete episodes of care for 7 common conditions following defined clinical pathways.
Accessing Pharmacy First services
The following table shows the 7 conditions pharmacists can manage across various age ranges.
| Clinical pathway | Age range |
| Acute otitis media* | 1 to 17 years |
| Impetigo | 1 year and over |
| Infected insect bites | 1 year and over |
| Shingles | 18 years and over |
| Sinusitis | 12 years and over |
| Sore throat | 5 years and over |
| Uncomplicated urinary tract infections | Women 16-64 years |
* Distance selling pharmacies will not complete consultations for acute otitis media.
Patients will be able to access the 7 clinical pathways element via referrals from referring organisations including general practice, urgent and emergency care settings, and NHS 111 (online and via telephone). In addition, for the 7 common conditions clinical pathway consultations only, patients can access the service by attending or contacting the pharmacy directly without the need for referral.
What happens next?
If you are being referred to your local pharmacy for other minor ailments *not one of the common conditions shown above. We will send your details and information about your condition to the pharmacy you have chosen.
You should call the pharmacy a few hours after you have been referred (if they haven’t already contacted you) to discuss next steps advising you were referred from your practice.
You will then have a consultation and be assessed by the pharmacist in a private consultation room.
How will the pharmacist help?
Pharmacists are highly skilled healthcare professionals who have trained for at least five years.
If the pharmacist reviews your symptoms and thinks you need to see another healthcare professional (eg GP, dentist, optician), they will help to arrange this.
The pharmacist can provide advice and reassurance on how to manage your condition, as many minor illnesses get better on their own. If the pharmacist thinks you need treatment to help with your symptoms, they may recommend an over-the-counter medicine.
If you are seeing them because you have run out of your usual medicine, they can help arrange a new supply.
The pharmacist will record the outcome of your consultation and send it to your GP to ensure your GP record is updated, including if any medicines are supplied.
Which pharmacy can I go to?
You can choose which pharmacy you go to, as long as it’s taking part in the scheme.
How will we use your information?
We will only use your personal information to help manage your care safely.
All of your personal information will be held securely by the NHS and will not be shared with third parties.
Health and Wellbeing Coaches
What is a Health and Wellbeing Coach?
A health and wellbeing coach can support you to improve how you manage your physical and mental health. They work with you through a series of sessions to help achieve your personalised health and care plan goals, offering support and advice about diet and lifestyle.
How can a health and wellbeing coach support me?
Health and wellbeing coaches support you to take proactive steps to improve the way you manage your physical and mental health conditions based on what matters to you.
They support you to develop knowledge, skills and confidence in managing your health and care, to improve your health and quality of life. They will coach and motivate you through multiple sessions to identify your needs, set goals and support you to achieve your personalised health are care objectives – providing interventions such as self-management education and peer support.
- 1:1 and group coaching
- Support setting personalised health goals
- Linking in with other services
- Support to manage your long-term health condition
- Support towards eating well, staying active or managing your weight
- Support to manage your mental wellbeing
- Adhere to a care plan
Where is a health and wellbeing coach based?
Health and wellbeing coaches are based within your local community. They work out of local GP surgeries so you may have an appointment at a different surgery to where you are registered.
How do I make an appointment to see a health and wellbeing coach?
Health and wellbeing coaches are accessible via your GP Surgery, when ringing for an appointment the reception team may suggest you speak to a health and wellbeing coach and a member of the team will then be in touch with more information and to find out if health coaching will be suitable for you. You can also make a self-referral by calling 01132405080.
What can I expect from an appointment with a health and wellbeing coach?
During the first session with a health and wellbeing coach they will find out more about you, your lifestyle, values, goals and anything that might get in the way of achieving those goals. You will then set some short-term goals that will enable you to start to work towards what it is you want to achieve. In the sessions that follow you will review your progress, set new goals and discuss any challenges you might have faced to help you overcome these in the future. In doing so, health coaching helps you develop the skills and confidence to manage your health and wellbeing.
Will I need to see a health and wellbeing coach on a regular basis?
You will be offered 6-8 sessions of support, consisting of 45-minute consultations via telephone, online or face-to-face.
Why is the health and wellbeing coach based at my GP surgery?
Primary care networks are prioritising the need for dedicated health and wellbeing provision within their primary care teams. The health and wellbeing coach works closely with the clinical staff in your GP practice to seek advice and guidance on different aspects of your care where necessary.
Cancer Care Coordinator
Around 20,800 people are diagnosed with cancer each year in Leeds and 55% of cancers are diagnosed early. Early diagnosis saves lives but screening uptake for breast, cervical and bowel cancers is often low. So, cancer screening is an important priority for our PCN.
Building on the previous ‘Cancer Wise Leeds’ programme (2019 – 2022) BHR PCN are now continuing the legacy work through the employment of a PCN Cancer Care Coordinator and Cancer Champions based in each of our 12 practices.
Cancer screening participation varies depending on multiple demographic and geographical factors. So, the aim is to have specific plans to target support to our population and patients that helps participation to reduce health inequalities.
The role of a Cancer Care Coordinator and cancer champions is to work closely with our patient population/ communities within our area to identify potential barriers to screening. Through this, we will be able to deliver information and education around screenings and tackle potential misconceptions.
What we know:
- Participation in bowel screening is low in deprived areas, and particularly South Asian communities.
- Participation in cervical screening is low in deprived areas, however there is variation in rates between ethnic groups.
- Breast screening is lowest in deprived areas and people from Black or South Asian backgrounds.
The cancer care coordinator will be supported by our colleagues in the PCN, working collaboratively to support our patients. We have a wide access to a variety of resources and want to make our patients feel comfortable and reassured to enable participation in cancer screening.
BHR PCN have a small dedicated team of healthcare assistants, nursing associates and care coordinators. They provide support to practices to identify and coordination care for a range of people, particularly those with long-term conditions and multiple long-term conditions. The team help people co-ordinate and navigate their care across the health and care system.
The approach is to provide support and influence the health of the community and its patients to tackle health inequalities.
Our population have a higher prevalence of long-term conditions particularly at an earlier age and because of the nature of our more deprived communities, along with our culturally diverse population, these multimorbidity patients are typically our hard-to-reach patients.
The team objectives is to support patients to stay well and manage their condition by working very closely with their GP’s.
Our Priority is Diabetes
What is diabetes? Find out in our two-minute video spoken in English. link: https://youtu.be/ZLOjD5IfUyU
Or choose a version in Urdu, Gujarati, Punjabi or Sylheti from our https://www.youtube.com/playlist?list=PLQDlTVSOXD9GeCq19dVbUpYZewQaztdsR
Our Focus area
Type 2 Diabetes in the Young Initiative
The National Diabetes Audit (NDA) shows that prevalence of type 2 diabetes in younger people is increasing yearly, with an estimated 137,260 people with type 2 diabetes aged 18-39 in England. In west Yorkshire prevalence is estimated at 7500 people; the majority of whom are cared for exclusively in General Practice (GP).
Diabetes in younger people is associated with a more aggressive diabetes phenotype than older-onset type 2 diabetes, including more rapid progression of glycaemia and early development of complications with significant reduction in life expectancy. Despite this, people with EOT2D are less likely to receive all NICE recommended care processes and tend to have higher HbA1c than older people with type 2 diabetes. The PCN LTC team are focused on supporting practices to target this population and improve health outcomes.
Type 2 Diabetes Path to Remission Programme
The NHS Type 2 Diabetes Path to Remission Programme is a joint initiative between NHS England and Diabetes UK. This programme provides a low calorie, total diet replacement treatment for people who are living with type 2 diabetes and obesity or overweight: the NHS Type 2 Diabetes Path to Remission Programme.
The programme is being offered to eligible people, participants will be offered low calorie, total diet replacement products including soups and shakes consisting of 800 to 900 kilocalories a day for 12 weeks. During this time, participants will replace all normal meals with these products. Alongside this, participants will receive support and monitoring for 12 months including help to re-introduce food after the initial 12-week period. This support will provide participants with the help and advice they need throughout every stage of the programme. The programme is fully funded by the NHS, therefore there is no cost to participants.
NHS Diabetes Prevention Programme
The NHS Diabetes Prevention Programme (NHS DPP) is a joint commitment from NHS England, Public Health England and Diabetes UK, to deliver at scale, evidence based behavioural interventions for individuals identified as being at high risk of developing Type 2 diabetes.
Start Your Journey to a Healther You Leaflet (wypartnership.co.uk) – Urdu
Start Your Journey to a Healther You Leaflet (wypartnership.co.uk) – Punjabi
The Health Population Management Hub
The BHR PCN has a dedicated team of healthcare assistants, nursing associates, and care coordinators who work within the Health Population Management Hub. Their role is to support practices in identifying and coordinating care for individuals, particularly those with, or at risk of, developing long-term conditions. The team helps patients navigate and coordinate their care across the health and care system, aiming to improve the health of the community and reduce health inequalities.
One of the team’s key objectives is to educate and support patients with prediabetes. Prediabetes occurs when blood sugar levels are higher than normal but not high enough for a diagnosis of type 2 diabetes. It is measured using a HbA1c test. This shows your average blood glucose (sugar) levels for the last two to three months.
People with prediabetes are at a higher risk of developing type 2 diabetes but often experience no symptoms. Medical terms for elevated blood sugar include:
- Impaired fasting glucose (IFG)
- Impaired glucose tolerance (IGT)
- Impaired glucose regulation (IGR)
- Non-diabetic hyperglycaemia
This video explains what your HbA1c result means:
Preventing Type 2 Diabetes
Research shows that combining lifestyle changes—such as improving diet, increasing physical activity, and achieving sustainable weight loss (if appropriate) can lower the risk of developing type 2 diabetes by around 50%. Being at risk doesn’t guarantee you’ll develop type 2 diabetes, but you can reduce your risk by making healthier choices in your diet and activity levels. Your healthcare team can support you in making these changes.
Managing Your Weight
If you are overweight or obese and at high risk of type 2 diabetes, even modest weight loss can be beneficial. Losing 5% of your body weight can significantly lower your risk. There are various ways to lose weight, and the key is finding the right support and strategies that work for you. If you need help managing your weight, a dietitian may be able to assist you. Your GP can also direct you to local weight management services.
Eating a Healthy, Balanced Diet
There’s no single “special diet” for people at risk of type 2 diabetes because everyone’s needs are different. However, the types of food we consume play a role in our risk. A diet high in sugar and carbohydrates and low in fibre content, is linked to an increased risk of developing type 2 diabetes. The good news is that by making healthier food choices, you can reduce this risk.
Healthy eating patterns linked with a lower risk of type 2 diabetes include:
- The Mediterranean diet – Mediterranean meal plan | Diabetes UK
- The Dietary Approaches to Stop Hypertension (DASH) diet – DASH diet – healthy eating that helps lower blood pressure
- Vegetarian and Vegan diets – The vegetarian diet – NHS / The vegan diet – NHS
- Reduced carbohydrate – Low-carb diet and meal plan | Eating with diabetes | Diabetes UK
These eating patterns emphasise healthy foods like fruits, vegetables, whole grains, and lean proteins. It’s the overall balance of your diet that plays a crucial role in keeping you healthy. To reduce your risk, aim to eat more foods linked with a lower risk, such as:
- Fruits and vegetables
- Whole grains (brown rice, wholemeal bread and whole wheat pasta)
- Beans and legumes
- Nuts and seeds
- Dairy e.g. Natural (Greek) yogurt and cheese
- Lean proteins (chicken, turkey) and fish
- Water, tea and coffee (unsweetened)
At the same time, reduce the intake of foods that are linked to a higher risk of type 2 diabetes, such as:
- Sugary drinks
- Red and processed meats (like beef, lamb, pork, ham, and sausages)
- Refined carbohydrates (such as sugary snacks, crisps, white bread, white rice, white pasta and sugary cereals)
- Potatoes (particularly French fries)
Be More Active
A sedentary lifestyle—spending long periods inactive—has been linked to an increased risk of type 2 diabetes. Increasing physical activity in your daily life can help lower your risk. You don’t have to join a gym or start a new sport. Small changes can make a difference. Try standing while taking phone calls, using stairs instead of the lift, doing chair exercises, or taking a walk during your lunch break.
By incorporating these small changes into your routine, you can make a big impact on your health and reduce your risk of type 2 diabetes.
NHS Diabetes Prevention Programme
The NHS Diabetes Prevention Programme (NHS DPP) is a joint commitment from NHS England, Public Health England and Diabetes UK, to deliver at scale, evidence based behavioural interventions for individuals identified as being at high risk of developing Type 2 diabetes.
Click here for more information – NHS Diabetes Prevention Information
Start Your Journey to a Healthier You Leaflet (wypartnership.co.uk) – Urdu
Start Your Journey to a Healther You Leaflet (wypartnership.co.uk) – Punjabi
Prediabetes Workshops
In addition to the NHS Diabetes Prevention Programme, the team will be running regular dedicated workshops aimed at patients who have been informed they have prediabetes in the last 12 months. These small group sessions will provide individuals with information about managing blood sugar levels alongside practical dietary and lifestyle advice. If you are interested in attending one of our workshops, please contact: 07355 674627
Appointment reminders for childhood immunisations are now also being used across the PCN in a number of different languages – for more information please select:
Children and Young People’s Social Prescribers
How we can help.
- Help and support with non-medical issues e.g., mental health, low school attendance, bullying, Primary School to High School transitioning, young carer support, managing challenging or risk-taking behaviour, NEET support (Not in Education, Employment or Training), Engaging patients with high repeat DNA’s where their health may be affected.
- Information on parent skills and classes
- Support with general well-being
- Digital Literacy support and SEND guidance.
- Support clients to access Health & Social Care where needed. This will include supporting patients at meetings and acting as advocates.
- Work with other third sector organisations in the community to break down barriers for patients and help them to access information they need.
Please refer through the orange triangle on the Child Health Hub tab.
Women’s Health Clinic
The Women’s Health Hub for Leeds has continued to expand work within the PCN. To date 20 outreach clinics have been offered to PCN patients offering faster access to gynaecology advice, treatment and if required referral for surgical interventions. These are women already referred to LTHT gynaecology services who are subsequently redirected to our clinic due to living in a BHR PCN postcode. This has enabled women in our PCN to be seen at around half the standard waiting time for gynaecology compared to that experienced for the rest of the city population. We are continuing to expand the clinical offer under the support of Dr Chipeta and are pleased to be joined by Dr Sian Taylor shortly allowing us to expand our GP clinical input. Our additional clinical aim for the remainder of 2024 is to commence a monthly gynaecology MDT for our PCN clinical teams with support from Dr Chipeta and Dr Spencer (Clinical Lead for Menopause Care). Details for this will be circulated shortly but we aim to offer an informal and supportive monthly session for discussion and learning around complex patients as well as an opportunity for education.
All the above clinical work is running in parallel with the patient support, education and advocacy arm of our Hub Project allowing women to access programmes focusing on menstrual health, PCOS, PMS and menopause. We would welcome any clinicians who would like to observe clinical or educational sessions so please do contact Dr Kathryn Hage if you have any queries. At present clinicians should continue to refer to all gynaecology services via normal routes as LTHT admin will subsequently allocate to our clinic if patients are suitable.
Menopause Groups
We are continuing to deliver Menopause groups, there is currently a three-week menopause group running. All aspects of menopause are covered from group discussions of physical and phycological effects of the menopause and support available. The peer support sharing in the sessions is quite remarkable. Molly Donavon the junior doctor working in the clinical Women’s Hub has joined the current menopause cohort group. Molly is a great asset in the sessions’ the ladies love her. Further work with Nick Millington from ‘Walk it Ride it ‘has offered patients a walking group this has been welcomed by several women from the group.
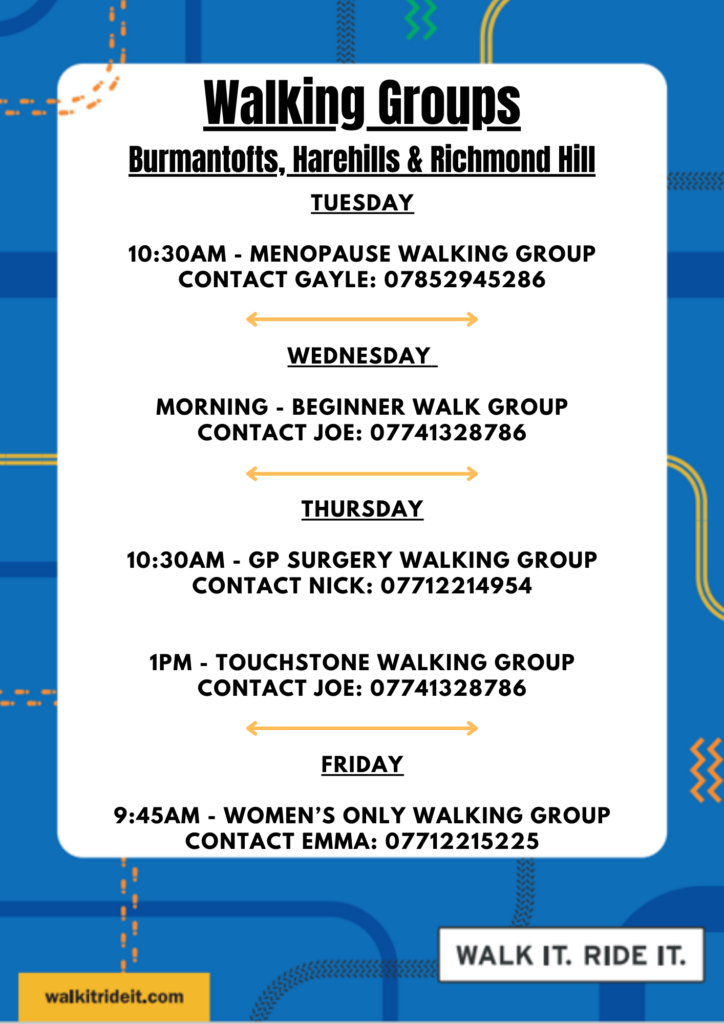
Walk It Ride It – Leeds
We’re making it easier for people to try free walking, wheeling, and cycling activities in Burmantofts, Harehills, and Richmond Hill.
Interested in cycling or walking more?
Spending time outside and moving around can help improve our mood, lower stress, and make us feel more relaxed.
Visit their website here for more information

HEALING, EDUCATION AND RECOVERY
OF EMOTIONAL STRENGTH
The HEROES mission is to support students to shine a light on, and shift, the limiting beliefs they have created about themselves and their identity, in response to the trauma they have encountered in their lives. The Programme works to hold a safe space for all members to build a better relationship with themselves and the world around them, for effective healing to occur.
Click HERE to learn more
The annual Learning disability health check was introduced into Primary care in 2006, The primary purpose of annual health checks is to address access and barriers experienced by people with a Learning Disability, furthermore, to allow the identification of unmet health needs. Health checks aim to improve prescribing and co-ordination with secondary care and identify any reasonable adjustment in accordance with the Disability Discrimination Act 1995.
People with a learning disability have poorer health and a lower life expectancy than the general population. They may not recognise that they are unwell or may be unable to communicate how they feel. They could also develop conditions or face challenges that are associated with their learning disability. The annual health checks for people with a learning disability differ from NHS health checks and include a more specific and detailed examination of a person’s physical and mental health. Carrying out these checks ensures that health issues are identified early, support can be provided promptly, and their health action plan is up to date.
Who is eligible?
Only patients with a diagnosed Learning disability age 14 and over are eligible for an annual review. Learning difficulties are not the same and patients with learning difficulty will not be eligible for an annual review.
A learning disability is a neurological condition that affects a person’s ability to process, understand, or retain information, which can make it challenging for them to learn new things or perform certain tasks. A learning disability will affect the way people learn new things throughout their life; it is a lifelong condition. Learning disabilities usually start in childhood but may not get diagnosed until adulthood. People with a learning disability may need support with understanding complex information, engaging with other people, and developing new skills.
Approximately 1.5 million people have learning disabilities in the UK.
Why is it important to attend an annual review?
Learning from Lives and Deaths (LeDeR), reviews deaths to see where we can find areas of learning, opportunities to improve, and examples of excellent practice. This information is then used to improve services for people living with a learning disability and autistic people.
Ledar Action from Learning each year around 41% of the Learning Disabilities UK population die of preventable diseases, according to LeDeR (Learning Disabilities Mortality Review NHS England), people with a learning disability often experience poorer health compared with the general population. The review investigates the deaths of people with a learning disability and revealed that on average, they die 20 years earlier than the rest of the population. They are also three times more likely to die from avoidable causes.
In 2006, the Disability Rights Commission recommended the introduction of annual health checks for people living with a learning disability in England and Wales.
Annual health checks are designed to promote healthy living and wellbeing, identify health issues early.
Useful links and easy read health information.
Get checked out – Learning Disability Service easy read format annual review information
learningdisabilityservice-leeds.nhs.uk
https://www.learningdisabilityservice-leeds.nhs.uk › get…
A safe space
The Compton Centre community hub. Harehills Lane Leeds LS9 … The building is a ‘Safe Place‘ for adults with a learning disability.
https://www.leeds.gov.uk › community-hubs › compton-…
Local learning disability groups and support services.
Learning Disability & Autism – People in Action (Yorkshire)
Leep1 – Supporting adults with learning disabilities to speak
Leeds Mencap – Learning Disability Charity – Leeds Mencap

Role of PCN Dietitian
The PCN Dietitian is a member of the healthcare team who works with GP practices within the PCN. Our PCN’s focus areas are Diabetes and Obesity.
Diabetes
The Dietitian can provide individualised dietary information for your patients with diabetes to help them manage their diet better and improve their diabetic control to reduce their risk of diabetic complications.
They will work with your patients to improve their knowledge and confidence by devising a dietary plan, set goals and review their progress.
Referral Criteria
- Adults aged 18 years plus.
- Patients with a diagnosis of Type 2 diabetes confirmed HbA1c >58, who have had at least one assessment with GP +/or Practice Nurse and require a dietary review to improve their HbA1c.
- Newly diagnosed Type 2 Diabetes (within the last 6 months) with HbA1c>48.
Exclusion criteria – (Not suitable for referral)
- Under 18 years old.
- Being seen by Community Diabetes team or hospital diabetes team.
- Patients with Type 1 Diabetes.
Obesity
The Dietitian can support your patients to build the knowledge, confidence and skills to achieve their health and weight management goals.
Referral Criteria
- Adults aged 18 years plus.
- Patients with a BMI over 35 under no other weight specialist care
Exclusion criteria – (Not suitable for referral)
- Under 18 years old.
- Or under weight management specialist team.
How to Refer
Please book your suitable patients into the PCN dietitian clinic appointment slots which are on the Confed Hub.
Please note it has been agreed the PCN Pharmacist team can task the Dietitian for advice around any Care Home patient’s dietetic issues.
Patients with Diabetes
Patient Information sheet to see PCN Dietitian
Role of PCN Dietitian
The PCN Dietitian is a member of the healthcare team who works with GP practices within the PCN in your local area. They can provide individualised dietary information for you, to help you manage your diet better and improve your diabetic control, to reduce your chance of developing other health problems due to your diabetes.
They will discuss your food and drink in detail and work with you to improve your knowledge and help you to manage your diabetic diet better. They will help you put together a dietary plan and set goals that you can work towards and then review your progress.
At your first appointment you will have a 45-minute telephone assessment and the Dietitian will decide the best way forward to review your progress. If appropriate, a further 30-minute follow up appointment will be arranged for you.
Who can see the PCN Dietitian?
- Adults aged 18 years plus.
- Patients with a diagnosis of Type 2 diabetes confirmed HbA1c over 58, who have had at least one assessment with GP +/or Practice Nurse and require a dietary review to improve their HBA1c.
- Newly diagnosed Type 2 Diabetes (within the last 6 months) with HbA1c>48.
Patients with high BMI
Patient Information sheet to see PCN Dietitian
Role of PCN Dietitian
The PCN Dietitian is a member of the healthcare team who works with GP practices within the PCN in your local area. They can support you to build the knowledge, confidence and skills to achieve your health and weight management goals.
They will discuss your food and drink in detail and can help you manage your diet better and reduce your chance of developing other health problems due to your weight.
They will help you put together a dietary plan and set goals that you can work towards and then review your progress.
At your first appointment you will have a 45-minute telephone assessment and the Dietitian will decide the best way forward to review your progress. If appropriate, a further 30-minute follow up appointment will be arranged for you.
Who can see the PCN Dietitian?
- Adults aged 18 years plus.
- Patients with a BMI over 35.
Oghuan Unuigbe works a hybrid model; face-to-face/telephone consultation on a Wednesday based at HC2 and remotely on a Friday.
* To book an appointment with the dietitian, please see rotas in the Confed hub.
Community NHS health checks
The Health Population Management Hub are currently offering NHS health checks at community events in the area to patients who are eligible and registered within the 12 practices.
What is an NHS health check?
The NHS Health Check is a free check-up of your overall health. It can tell you whether you’re at higher risk of getting certain health problems, such as:
- Heart disease
- Diabetes
- kidney disease
- Stroke
If you’re aged over 65, you’ll also be told about symptoms of dementia to look out for.
Are you Eligible?
The check is for people who are aged 40 to 74 who do not have any of the following pre-existing conditions:
- Heart disease
- Chronic kidney disease
- Diabetes – pre diabetes
- High Blood Pressure (hypertension)
- Atrial Fibrillation
- Transient ischaemic attack
- Inherited high cholesterol (familial hypercholesterolemia)
- Heart failure
- Peripheral arterial disease
- Stroke
Or currently being prescribed statins to lower cholesterol
What Happens during an NHS health check
During your NHS health check the following will happen
- Height, weight and waist measurement
- Blood pressure reading
- Cholesterol test using Point of care testing.
- Family history
- Diet and lifestyle questions.
All of this helps to work out your Q-risk score. This will tell you your risk of developing cardiovascular disease in the next 10 years.
What is point of care testing?
Point of care testing is a type of test that allows for immediate results.
A small sample of blood is taken from the finger. The test is then analysed, and results are available within a short period of time.
Watch our video to find out more about what happens during a community NHS health check.